An award-winning cannabis podcast for women, by women. Hear joyful stories and useful advice about cannabis for health, well-being, and fun—especially for needs specific to women like stress, sleep, and sex. We cover everything from: What’s the best weed for sex? Can I use CBD for menstrual cramps? What are the effects of the Harlequin strain or Gelato strain? And, why do we prefer to call it “cannabis” instead of “marijuana”? We also hear from you: your first time buying legal weed, and how ...
…
continue reading
Content provided by PulmPEEPs. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by PulmPEEPs or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://ppacc.player.fm/legal.
Similar to PulmPEEPs
Everyone has a dream. But sometimes there’s a gap between where we are and where we want to be. True, there are some people who can bridge that gap easily, on their own, but all of us need a little help at some point. A little boost. An accountability partner. A Snooze Squad. In each episode, the Snooze Squad will strategize an action plan for people to face their fears. Guests will transform their own perception of their potential and walk away a few inches closer to who they want to become ...
…
continue reading
Interviews with mathematics education researchers about recent studies. Hosted by Samuel Otten, University of Missouri. www.mathedpodcast.com Produced by Fibre Studios
…
continue reading
Are you looking for more happiness, success and vitality in your life? Get inspired each week with wellness and performance expert, Integrative Medicine Fellow, author & keynote speaker, Kristel Bauer. Live Greatly shares empowering conversations and insights about happiness, wellness & success to support your personal and professional development. Kristel talks with top experts, leaders and inspiring individuals to help you embrace a growth mindset and excel in your work/life. Kristel then ...
…
continue reading
A science guy from the deep south (Destin) and a humanities guy from the wild west (Matt Whitman) discuss deep questions with varying levels of maturity.
…
continue reading
1
Españolistos | Learn Spanish With Fun Conversations!
Españolistos | Learn Spanish With Fun Conversations!
Españolistos is a Spanish language learning Podcast spoken in clear Latin American Spanish geared towards intermediate to advanced language learners. The conversations are 99% in Spanish so you can focus on your listening comprehension. The topics are fun and interesting, sometimes controversial, and always educational. We believe that discussing deep and meaningful topics will increase your vocabulary as you learn new and practical words for everyday living. Andrea (Colombian Spanish Teache ...
…
continue reading
1
Every Day Is Saturday Podcast For Motivation, Inspiration And Success
Self Improvement Coach Sam Crowley
One of the top motivational podcasts for 18 years and running. Motivational messages to keep you inspired throughout the week. Success comes in all shapes and sizes. Sam Crowley’s authentic message will provide the inspiration you need to conquer the challenges and claim your power.
…
continue reading
(Apple's Best of 2018) In-depth conversations with people at the top of their game. Jordan Harbinger unpacks guests' wisdom into practical nuggets you can use to impact your work, life, and relationships. Learn from leaders (Ray Dalio, Simon Sinek, Mark Cuban), entertainers (Moby, Tip "T.I." Harris, Dennis Quaid), scientists (Neil deGrasse Tyson, Bill Nye), athletes (Kobe Bryant, Dennis Rodman, Tony Hawk) and an eclectic array of fascinating minds, from art forgers and arms traffickers to sp ...
…
continue reading
BackStory is a weekly public podcast hosted by U.S. historians Ed Ayers, Brian Balogh, Nathan Connolly and Joanne Freeman. We're based in Charlottesville, Va. at Virginia Humanities. There’s the history you had to learn, and the history you want to learn - that’s where BackStory comes in. Each week BackStory takes a topic that people are talking about and explores it through the lens of American history. Through stories, interviews, and conversations with our listeners, BackStory makes histo ...
…
continue reading
Do you think it's possible to reach your potential in just minutes a day? Hundreds of thousands of people have turned to Self Improvement Daily to get the encouragement, inspiration, and competitive edge they need to do become the best version of themselves! The podcast helps you prioritize personal development in a way that is practical, doable, and highly effective. Instead of feeling like life is passing you by, you will start showing up to every moment with more enthusiasm and confidence ...
…
continue reading
Player FM - Podcast App
Go offline with the Player FM app!
Go offline with the Player FM app!

))
97. Rapid Fire Journal Club – MIST 2
Manage episode 475776467 series 3299598
Content provided by PulmPEEPs. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by PulmPEEPs or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://ppacc.player.fm/legal.
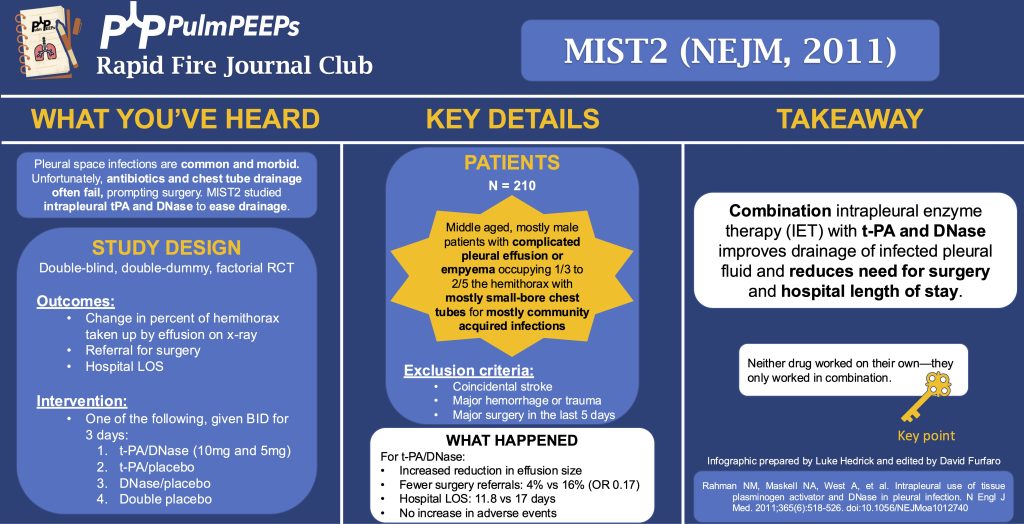
In this episode, we add another article to our Rapid Fire Journal Club. Luke Hedrick and Dave Furfaro discuss the MIST 2 trial published in NEJM in 2011 evaluating enzymatic therapy for complex parapneumonic effusions and empyemas.

Article and Reference
We are talking today about the MIST 2 trial evaluating the use of intrapleural tPa and DNase for intrapleural infections.
Key Learning Points
-
- Background:
- Infections in the pleural space are common and morbid, often requiring surgical intervention. Unfortunately, antibiotics and chest tube drainage often fail. The MIST1 trial (NEJM, 2005) of intrapleural streptokinase showed no benefit. MIST2 studied intrapleural tPA and DNase to ease drainage by breaking down septations and thinning pleural fluid.
- Study Design (design, primary outcome, participants, etc)
- Design:
- Double-blind, double-dummy, 2×2 factorial RCT at 11 UK hospitals from 12/2005 to 11/2008
- By double dummy, we mean that there was a sham placebo for each of the study drugs
- Double-blind, double-dummy, 2×2 factorial RCT at 11 UK hospitals from 12/2005 to 11/2008
- Primary Outcome
- Change in the percent of the hemithorax taken up by effusion on CXR at day 7 compared to day 1
- Key secondary outcomes:
- Referral for surgery
- Hospital LOS
- All cause 3 month and 12 month mortality
- AEs
- Participants
- Inclusion:
- Clinical evidence of infection (assessed by recruiting MD; EG, fever, CRP, WBC) and
- Pleural fluid with any of:
- Grossly purulent
- Positive pleural fluid culture or gram stain
- pH < 7.2
- Exclusion: aiming to exclude patients with increased bleeding risk or who can’t re-expand the lung after drainage
- Age < 18
- Previous intrapleural fibrinolytics, DNase, or both for empyema
- Allergy to tPA or DNase
- Coincidental stroke (hemorrhage risk)
- Major hemorrhage or trauma
- Major surgery in the last 5 days
- Previous pneumonectomy on the infected side
- Pregnancy, lactation
- Expected survival < 3 months from something other than what caused the pleural problem
- Summary: Middle-aged, mostly male patients with complicated pleural effusion or empyema occupying 1/3 to 2/5 hemithorax with mostly small-bore CDs for mostly community-acquired infections
- Inclusion:
- Design:
- Background:
Small-bore here meant < 15 Fr
- Intervention/Limitations
- N = 210 (193 analyzed) randomized approximately 1:1 to one of the following 4 arms:
- tPA/Dnase (10mg and 5mg)
- tPA and placebo
- DNase and placebo
- Double placebo
- N = 210 (193 analyzed) randomized approximately 1:1 to one of the following 4 arms:
-
-
- Medications were given BID for 3 days with clamping of the CD for 1 hour after each dose (to keep the drug in the pleural space)
-
- Outcomes/Safety
- Power: with N = 210 (actual analysis = 193), 80% power to detect 1 in 5 more patients with a 50% reduction in pleural opacity on CXR
- We’ll discuss the outcomes of tPA/DNase in combination because there was a highly significant interaction between the two (P = 0.002) for the primary outcome
- Efficacy:
-
-
- Primary (pleural effusion size reduction): -29.5% hemithorax vs baseline and -7.9% effusion size vs placebo (P = 0.005)
- Neither drug worked on their own
- Secondary:
- Referral for surgery: 4% vs 16% (OR 0.17, P = 0.03)
- Hospital LOS (excluding 391d outlier in placebo group): mean 11.8 vs 17 days (P = 0.006)
- Mortality: no difference
- Primary (pleural effusion size reduction): -29.5% hemithorax vs baseline and -7.9% effusion size vs placebo (P = 0.005)
-
-
- Safety:
-
-
- No difference in AE between groups
- 6 serious events across all groups, mostly related to bleeding (intra-pleural, GI, hemoptysis); other AE were made up of pain with drug administration, transient AMS, rash
-
- Takeaway
- Combination intrapleural enzyme therapy (IET) with tPA and DNase improves drainage of infected pleural fluid, and reduces need for surgery and hospital LOS
Infographic
102 episodes
Manage episode 475776467 series 3299598
Content provided by PulmPEEPs. All podcast content including episodes, graphics, and podcast descriptions are uploaded and provided directly by PulmPEEPs or their podcast platform partner. If you believe someone is using your copyrighted work without your permission, you can follow the process outlined here https://ppacc.player.fm/legal.
In this episode, we add another article to our Rapid Fire Journal Club. Luke Hedrick and Dave Furfaro discuss the MIST 2 trial published in NEJM in 2011 evaluating enzymatic therapy for complex parapneumonic effusions and empyemas.
Article and Reference
We are talking today about the MIST 2 trial evaluating the use of intrapleural tPa and DNase for intrapleural infections.
Key Learning Points
-
- Background:
- Infections in the pleural space are common and morbid, often requiring surgical intervention. Unfortunately, antibiotics and chest tube drainage often fail. The MIST1 trial (NEJM, 2005) of intrapleural streptokinase showed no benefit. MIST2 studied intrapleural tPA and DNase to ease drainage by breaking down septations and thinning pleural fluid.
- Study Design (design, primary outcome, participants, etc)
- Design:
- Double-blind, double-dummy, 2×2 factorial RCT at 11 UK hospitals from 12/2005 to 11/2008
- By double dummy, we mean that there was a sham placebo for each of the study drugs
- Double-blind, double-dummy, 2×2 factorial RCT at 11 UK hospitals from 12/2005 to 11/2008
- Primary Outcome
- Change in the percent of the hemithorax taken up by effusion on CXR at day 7 compared to day 1
- Key secondary outcomes:
- Referral for surgery
- Hospital LOS
- All cause 3 month and 12 month mortality
- AEs
- Participants
- Inclusion:
- Clinical evidence of infection (assessed by recruiting MD; EG, fever, CRP, WBC) and
- Pleural fluid with any of:
- Grossly purulent
- Positive pleural fluid culture or gram stain
- pH < 7.2
- Exclusion: aiming to exclude patients with increased bleeding risk or who can’t re-expand the lung after drainage
- Age < 18
- Previous intrapleural fibrinolytics, DNase, or both for empyema
- Allergy to tPA or DNase
- Coincidental stroke (hemorrhage risk)
- Major hemorrhage or trauma
- Major surgery in the last 5 days
- Previous pneumonectomy on the infected side
- Pregnancy, lactation
- Expected survival < 3 months from something other than what caused the pleural problem
- Summary: Middle-aged, mostly male patients with complicated pleural effusion or empyema occupying 1/3 to 2/5 hemithorax with mostly small-bore CDs for mostly community-acquired infections
- Inclusion:
- Design:
- Background:
Small-bore here meant < 15 Fr
- Intervention/Limitations
- N = 210 (193 analyzed) randomized approximately 1:1 to one of the following 4 arms:
- tPA/Dnase (10mg and 5mg)
- tPA and placebo
- DNase and placebo
- Double placebo
- N = 210 (193 analyzed) randomized approximately 1:1 to one of the following 4 arms:
-
-
- Medications were given BID for 3 days with clamping of the CD for 1 hour after each dose (to keep the drug in the pleural space)
-
- Outcomes/Safety
- Power: with N = 210 (actual analysis = 193), 80% power to detect 1 in 5 more patients with a 50% reduction in pleural opacity on CXR
- We’ll discuss the outcomes of tPA/DNase in combination because there was a highly significant interaction between the two (P = 0.002) for the primary outcome
- Efficacy:
-
-
- Primary (pleural effusion size reduction): -29.5% hemithorax vs baseline and -7.9% effusion size vs placebo (P = 0.005)
- Neither drug worked on their own
- Secondary:
- Referral for surgery: 4% vs 16% (OR 0.17, P = 0.03)
- Hospital LOS (excluding 391d outlier in placebo group): mean 11.8 vs 17 days (P = 0.006)
- Mortality: no difference
- Primary (pleural effusion size reduction): -29.5% hemithorax vs baseline and -7.9% effusion size vs placebo (P = 0.005)
-
-
- Safety:
-
-
- No difference in AE between groups
- 6 serious events across all groups, mostly related to bleeding (intra-pleural, GI, hemoptysis); other AE were made up of pain with drug administration, transient AMS, rash
-
- Takeaway
- Combination intrapleural enzyme therapy (IET) with tPA and DNase improves drainage of infected pleural fluid, and reduces need for surgery and hospital LOS
Infographic
102 episodes
All episodes
×Welcome to Player FM!
Player FM is scanning the web for high-quality podcasts for you to enjoy right now. It's the best podcast app and works on Android, iPhone, and the web. Signup to sync subscriptions across devices.
Similar to PulmPEEPs
An award-winning cannabis podcast for women, by women. Hear joyful stories and useful advice about cannabis for health, well-being, and fun—especially for needs specific to women like stress, sleep, and sex. We cover everything from: What’s the best weed for sex? Can I use CBD for menstrual cramps? What are the effects of the Harlequin strain or Gelato strain? And, why do we prefer to call it “cannabis” instead of “marijuana”? We also hear from you: your first time buying legal weed, and how ...
…
continue reading
Everyone has a dream. But sometimes there’s a gap between where we are and where we want to be. True, there are some people who can bridge that gap easily, on their own, but all of us need a little help at some point. A little boost. An accountability partner. A Snooze Squad. In each episode, the Snooze Squad will strategize an action plan for people to face their fears. Guests will transform their own perception of their potential and walk away a few inches closer to who they want to become ...
…
continue reading
Interviews with mathematics education researchers about recent studies. Hosted by Samuel Otten, University of Missouri. www.mathedpodcast.com Produced by Fibre Studios
…
continue reading
Are you looking for more happiness, success and vitality in your life? Get inspired each week with wellness and performance expert, Integrative Medicine Fellow, author & keynote speaker, Kristel Bauer. Live Greatly shares empowering conversations and insights about happiness, wellness & success to support your personal and professional development. Kristel talks with top experts, leaders and inspiring individuals to help you embrace a growth mindset and excel in your work/life. Kristel then ...
…
continue reading
A science guy from the deep south (Destin) and a humanities guy from the wild west (Matt Whitman) discuss deep questions with varying levels of maturity.
…
continue reading
1
Españolistos | Learn Spanish With Fun Conversations!
Españolistos | Learn Spanish With Fun Conversations!
Españolistos is a Spanish language learning Podcast spoken in clear Latin American Spanish geared towards intermediate to advanced language learners. The conversations are 99% in Spanish so you can focus on your listening comprehension. The topics are fun and interesting, sometimes controversial, and always educational. We believe that discussing deep and meaningful topics will increase your vocabulary as you learn new and practical words for everyday living. Andrea (Colombian Spanish Teache ...
…
continue reading
1
Every Day Is Saturday Podcast For Motivation, Inspiration And Success
Self Improvement Coach Sam Crowley
One of the top motivational podcasts for 18 years and running. Motivational messages to keep you inspired throughout the week. Success comes in all shapes and sizes. Sam Crowley’s authentic message will provide the inspiration you need to conquer the challenges and claim your power.
…
continue reading
(Apple's Best of 2018) In-depth conversations with people at the top of their game. Jordan Harbinger unpacks guests' wisdom into practical nuggets you can use to impact your work, life, and relationships. Learn from leaders (Ray Dalio, Simon Sinek, Mark Cuban), entertainers (Moby, Tip "T.I." Harris, Dennis Quaid), scientists (Neil deGrasse Tyson, Bill Nye), athletes (Kobe Bryant, Dennis Rodman, Tony Hawk) and an eclectic array of fascinating minds, from art forgers and arms traffickers to sp ...
…
continue reading
BackStory is a weekly public podcast hosted by U.S. historians Ed Ayers, Brian Balogh, Nathan Connolly and Joanne Freeman. We're based in Charlottesville, Va. at Virginia Humanities. There’s the history you had to learn, and the history you want to learn - that’s where BackStory comes in. Each week BackStory takes a topic that people are talking about and explores it through the lens of American history. Through stories, interviews, and conversations with our listeners, BackStory makes histo ...
…
continue reading
Do you think it's possible to reach your potential in just minutes a day? Hundreds of thousands of people have turned to Self Improvement Daily to get the encouragement, inspiration, and competitive edge they need to do become the best version of themselves! The podcast helps you prioritize personal development in a way that is practical, doable, and highly effective. Instead of feeling like life is passing you by, you will start showing up to every moment with more enthusiasm and confidence ...
…
continue reading
Player FM - Podcast App
Go offline with the Player FM app!
Go offline with the Player FM app!